


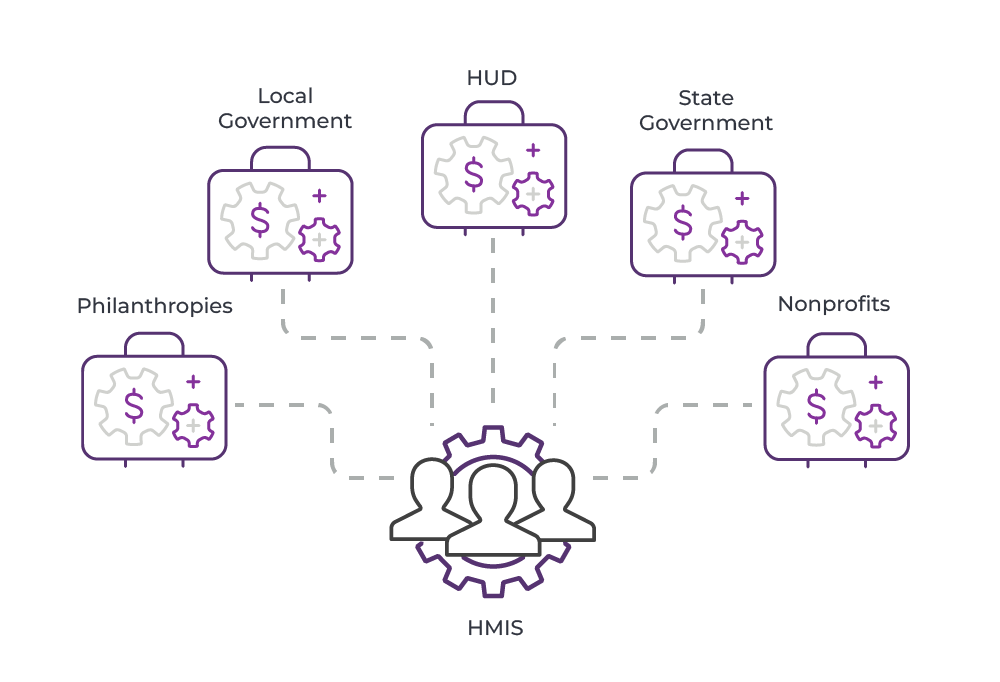

 Organization
OrganizationThe challenge is to marry the practitioner’s experience and intuition with data science. Those who oversee HMISes within each CoC now need to move faster to adapt to emerging trends in technology. For example, many forward-thinking HMIS administrators have experience as business-systems analysts, data-quality specialists, system administrators, and the like.
To be clear, there is no “normal” standard yet for HMIS administration, but there is a convergence forming around the skills necessary to use data (i.e., data mining, data analysis). However, HMIS administrators should have a working knowledge of public policy. After all, it wasn’t until 2004 when the HMIS Data Standards were instituted by HUD.
Best Practice: Continuing Education for the HMIS
Every HMIS lead comes to this role from a different career path, so there’s a real need for administrators to learn from each other. More data-competent leads would do well to learn more about public policy and socio-cultural factors in homelessness, for example. More policy-competent leads would benefit from learning more about data analysis.
Recommended to attend (HMIS specific):
- National Human Services Data Consortium
- National Alliance to End Homelessness
- National Health Care for the Homeless Council
Learning and development software can also be very beneficial for HMIS and CoC users at all levels of the organization, which is why Eccovia has now developed Eccovia University, an L&D platform specifically created for social service organizations.
 Technology
TechnologyTraditional Data Integration
What happens when service providers don’t share data? You get duplicated efforts, increased inefficiencies in provision of services, and wasted money. Most important, your client outcomes aren’t going to be what they could be. That’s why we emphasize that compliance isn’t enough to mitigate homelessness.
It’s becoming increasingly clear that preventing homelessness can be done when programs and social service providers work together in a centralized data platform. For example, reformed convicts in the United Kingdom are more likely to commit another crime within one year when they’re unhoused. The Corporation for Supportive Housing (CSH) published a report detailing a few cases where data integration, between corrections departments and providers, facilitated supportive housing for ex-offenders after finishing their sentences, which proved to help mitigate their risk of homelessness.
Best Practice: Data Integration from Various Sources
Data integration is how care providers link together when they serve the same populations. Often, HMISes and CoCs believe that data integration with historical data is enough, but what about other nontraditional data sources (i.e., economic, weather, transactional, health, behavioral) that also affect unhoused populations? It’s increasingly essential for community intelligence to be married with community care. For example, a medical provider treating clients of social providers should be collaborating with those providers.
To that end, we’ve created an AI-powered data warehouse for social service delivery, ClientInsight. While the attempt of Stellas is noble, ClientInsight can gather, ingest, and process cross-organizational and nontraditional data, while Stellas can only work on HMIS data.
Data warehouses are becoming more popular for social services. While well intentioned, Stella P and Stella M—HUD’s frameworks for system modeling and systems analysis—are not the total solution because they’re not flexible enough to be used how HUD intended, in many circumstances. After all, with Stella P, you’re basically exporting a CSV file, rather than leveraging that data for data visualization and business (or community) intelligence.
In other words, the regulatory frameworks from HUD are only one piece of the puzzle. If you’re going to the trouble of negotiating data-sharing agreements and evaluating data sources with other providers, you might as well get a data warehouse. It would be a monumental undertaking to get those agreements and then manually maintain those data environments.
Communication Between Providers
Aside from the most technologically advanced CoCs, most CoCs communicate via email and phone. While not inherently wrong, case-specific communication via traditional methods can often get lost on a client profile when multiple providers have their own systems.
Some case workers can infer what clients need without having to call or email other providers, but when the data is siloed and care isn’t coordinated, you have to know to ask whether the client is being served at other agencies.
 Best Practice: Synchronized Communication
Best Practice: Synchronized CommunicationWhat if that communication could be streamlined? What if case workers could infer clients’ needs without having to call or email other providers? It might seem like a pipe dream, but it’s very possible with case management systems like ClientTrack, which breaks down the barriers separating data silos and impeding whole person care with a single source of truth that links all providers, matching clients to needed services.
 Services to CoCs
Services to CoCs Best Practice: Listen and Include Stakeholders in Training Curriculum
Because CoCs are composed of myriad organizations that have widely varied skillsets and goals, your training should reflect the knowledge and skills identified by the stakeholders. For example, if your local department of corrections is not equipped to evaluate needs of inmates about to finish their sentences, you can help correct this blind spot.
Data Quality Analysis
HMISes are also responsible for a laundry list of federal reports. Some communities will even issue report cards that have to be compiled, graded, and distributed. More technically advanced communities will automate these performance assessments, but they often have to be done manually on a monthly basis.
What caseworker can honestly say she has the time to go row by row to validate the data fields entered against the requirements? Many CoCs will even just “eyeball it” and try to deduplicate records where they see them, but who knows how many missing values get through the cracks in those cases, skewing the aggregate data?
Best Practice: Evaluate Data Quality
Stakeholders in your HMIS need to know what “good” data quality looks like. That’s why HMIS administrators need to perform due diligence that includes all stakeholders, while providing timely updates on changing data quality throughout the HMIS.
 Processes
ProcessesHMISes and CoCs have coordinated entry, a best practice for responding to people experiencing homelessness. However, for coordinated entry to happen, there must be an intake.
Intake can’t be defined easily: there are about 14 types of housing and HUD projects in the United States, and the differences between them are often nuanced and plentiful. For example, there are two types of emergency shelter as defined by HUD, transitional housing, different types of permanent housing, grant per diem (GPD), HOPWA, and Ryan White.
Partly because of the many types of housing support available, HUD (and other regulatory entities) require a high level of data during intake. Many social workers will feel this level of data intrusive, perhaps even traumatizing to clients or vicariously to themselves.
To quote a recent article we wrote:
- After all, questions like, “Have you ever been raped?” or, “Have you ever committed sex acts in exchange for money or food?” can have an emotional cost to both the client and the worker performing the intake.
Psychologist Stephen Fleming, a world-renowned trauma researcher, writes, “One need not directly experience or observe an event for it to be potentially traumatic; events experienced by others that one learns about also have this potential.”
The operative word there is “potential.” In a recent interview, Fleming states he prefers to use the term “potentially traumatic event” (PTE) because it doesn’t assume trauma or PTSD symptoms, as many people can experience PTEs without any PTSD symptoms.
On that same vein, potential harm can be caused when the intake worker assumes the new client must have been traumatized, which can prime that individual with a false narrative of how they “should” have reacted to the PTE.
That said, reliving old PTEs can also cause temporary emotional distress. So that’s where the debate lives right now: do we cause more potential harm by not collecting enough data or by collecting too much?
The fact that the United States has a threshold on spending toward vulnerable populations isn’t likely to change. Therefore, we still need a lot of that data.
Best Practice: Learn and Demonstrate Trauma Sensitivities
The client expectations might be different, depending on the nature of the service program. Shelter intake will be different from coordinated entry intake, so the intake questions will be varied. Case workers performing intake will necessarily ask a lot of intrusive questions, and some potential clients will find this process painful or triggering.
The Substance Abuse and Mental Health Services Administration (SAMHSA) calls the trauma-informed approach the Four R’s:
- Realize the impact of trauma and the potential paths to recovery;
- Recognize the signs and symptoms of trauma in clients;
- Respond with policies that integrate knowledge about trauma; and,
- Resist retraumatization when asking intake questions.
Service Provision
Fair distribution of services is a challenge for most CoCs and HMISes because what’s fair is a debate of ethics. Really advanced communities are pulling data like demographics, income, race, and the like to determine whether there’s a potential bias, but many service providers tend to struggle with this question of fairness.
That’s why system mapping is a useful exercise to follow where the services are being used most, but it’s extremely labor intensive and difficult to do manually. That’s one reason community-intelligence platforms like ClientInsight can provide greater efficiency and accuracy.
In short, we need an analytics revolution in social services.
Best Practice: Closed-Loop Referral
The initiator of the service request should be able to identify the provider and notify them before the client arrives or contacts the provider, passing along any documentation that was part of the referral. The agency then receives the referral, and the “loop” is “closed” when the client (ideally) shows up or there is a result indicated. Even “failed” or “ineligible” results can be a long-term silver lining, because at least that data helps improve the system.
ClientTrack facilitates this process with an eligibility engine and closed-loop referral workflow.
Exit and After-care
The line between traditional homeless management information systems (i.e., data points about support for homeless populations) and modern HMISes is becoming blurrier. The most forward-thinking HMISes now track after-care and have exit strategies in place for clients beyond providing permanent housing. That said, a successful exit to permanent housing is what is measured by HUD.
How do most clients leave an HMIS?
- Sometimes, clients suddenly disappear and lose contact with service providers. Others just leave for a period of time and come back.
- Sometimes, it’s a transitional housing project and the client fails out of it.
- Sometimes, the individual is sent to a substance treatment facility.
- Sometimes, there’s criminal activity that can’t be addressed through a harm-reduction model because of client behavior.
- Sometimes, clients pass away.
What does stability look like for HMISes and their clients?
Placing a client in permanent housing is not always successful. Some case managers will look for opportunities for clients to be reunified with their families, which could be the best outcome in many cases, especially where medical noncompliance for a severe psychiatric illness is an issue.
For HUD, the desired outcome is housing. However, case workers often need to maintain a connection with clients to mitigate recidivism. One helpful practice to supplement the case worker–client relationship is to place housed, former clients as peer mentors for new clients entering the CoC’s system.
After-care matters because HUD also wants to see a reduction in recidivism. The follow-up relationship helps ensure stability. In a data warehouse environment, you bring in other data sources from public services not in the CoC (i.e., unemployment offices, Social Security, housing assistance, SNAP) and share that data across the CoC for the benefit of case managers. However, it’ll probably be a more gradual process to get data-sharing agreements with those public services that aren’t specifically geared toward homeless populations.
Best Practice: Automate Processes Where Possible
Automation is not the same thing as “not caring” or “disinterest.” The reality is there is not enough time, capacity, or workforce to handle the amounts of cases in many communities. So, in many instances, it might come down to either choosing an automated, follow-up robo-call and, well, nothing. In that case, it’s better to automate the robo-call, albeit less intimate.
The principle is this: if left to short-term memory, many follow-ups can easily be forgotten. Human frailty in the CoC must be mitigated where possible.

